Physical Therapy For Calcaneal Apophysitis
Overview
Sever's disease or Calcaneal apophysitis is a condition that affects children between the ages of 10 and 13 years. It is characterized by pain in one or both heels with walking. During this phase of life, growth of the bone is taking place at a faster rate than the tendons. Hence there is a relative shortening of the heel-cord compared to the leg bones. As a result, the tension the heel-cord applies to the heel bone at its insertion is very great. Moreover, the heel cord is attached to a portion of the calcaneus (heel bone) that is still immature, consisting of a mixture of bone and growing cartilage, called the calcaneal apophysis, which is prone to injury. Compounding to this is the fact that all these changes are happening in a very active child, prone to overuse. The end result is therefore an overuse syndrome of injury and inflammation at the heel where the heel cord (Achilles Tendonitis) inserts into the heel bone (Calcaneal apophysitis).
Causes
Sever?s disease is often associated with a growth spurt, when the bones grow but the muscles do not. Therefore the muscles effectively become tighter which results in increased stress at the heel. It may also be related to unusual biomechanics, for instance poor foot posture, muscle tightness or muscle weakness. Overtraining or incorrect training can also play a part. Usually, the cause is a combination of factors.
Symptoms
Pain is usually felt at the back of the heel and around the sides of the heel. If you squeeze the back of the heel from both sides simultaneously and pain is experienced Sever?s disease is more than likely present.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
If the problem is bad enough, it is important to totally rest the symptomatic foot. Take a break from sport activity until the pain has significant improvement. Severe cases will need to be treated with a cast boot. Anti-inflammatory treatments include Icing, Over-the-counter anti-inflammatory medicine as recommended by your pediatrician or podiatrist. Shock absorption and support. Don't go barefoot at home, wear some type of good sandal or shoe. A significant and/or chronic case should be treated with prescription orthotics. This addresses mechanical problems that cause this problem, Using an over-the-counter heel cushion inside of the shoe, Athletic foot taping, Stretching. Runners stretch to stretch out the calf muscle. A night splint will also help. Severe or chronic cases respond best to prescription orthotics with specific modifications for this problem. May require a night splint. Daytime braces that may also help.
Prevention
To reduce the risk of heel pain or sore heels from Sever?s Disease. Only wear properly fitting shoes. A lace up shoe with a firm heel counter. Stretch calf and foot before exercising or playing sports. Properly taping the foot provides excellent protection and immediate pain relief. Wear shoe inserts or an over-the-counter orthotic. If the problem persists, consult your foot doctor.
Sever's disease or Calcaneal apophysitis is a condition that affects children between the ages of 10 and 13 years. It is characterized by pain in one or both heels with walking. During this phase of life, growth of the bone is taking place at a faster rate than the tendons. Hence there is a relative shortening of the heel-cord compared to the leg bones. As a result, the tension the heel-cord applies to the heel bone at its insertion is very great. Moreover, the heel cord is attached to a portion of the calcaneus (heel bone) that is still immature, consisting of a mixture of bone and growing cartilage, called the calcaneal apophysis, which is prone to injury. Compounding to this is the fact that all these changes are happening in a very active child, prone to overuse. The end result is therefore an overuse syndrome of injury and inflammation at the heel where the heel cord (Achilles Tendonitis) inserts into the heel bone (Calcaneal apophysitis).
Causes
Sever?s disease is often associated with a growth spurt, when the bones grow but the muscles do not. Therefore the muscles effectively become tighter which results in increased stress at the heel. It may also be related to unusual biomechanics, for instance poor foot posture, muscle tightness or muscle weakness. Overtraining or incorrect training can also play a part. Usually, the cause is a combination of factors.
Symptoms
Pain is usually felt at the back of the heel and around the sides of the heel. If you squeeze the back of the heel from both sides simultaneously and pain is experienced Sever?s disease is more than likely present.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
If the problem is bad enough, it is important to totally rest the symptomatic foot. Take a break from sport activity until the pain has significant improvement. Severe cases will need to be treated with a cast boot. Anti-inflammatory treatments include Icing, Over-the-counter anti-inflammatory medicine as recommended by your pediatrician or podiatrist. Shock absorption and support. Don't go barefoot at home, wear some type of good sandal or shoe. A significant and/or chronic case should be treated with prescription orthotics. This addresses mechanical problems that cause this problem, Using an over-the-counter heel cushion inside of the shoe, Athletic foot taping, Stretching. Runners stretch to stretch out the calf muscle. A night splint will also help. Severe or chronic cases respond best to prescription orthotics with specific modifications for this problem. May require a night splint. Daytime braces that may also help.
Prevention
To reduce the risk of heel pain or sore heels from Sever?s Disease. Only wear properly fitting shoes. A lace up shoe with a firm heel counter. Stretch calf and foot before exercising or playing sports. Properly taping the foot provides excellent protection and immediate pain relief. Wear shoe inserts or an over-the-counter orthotic. If the problem persists, consult your foot doctor.
Posterior Tibial Tendon Dysfunction Surgery Success
Overview
Adult flatfoot refers to a deformity that develops after skeletal maturity is reached. Adult flatfoot should be differentiated from constitutional flatfoot, which is a common congenital non-pathologic foot morphology. There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. 
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder.
Symptoms
The first stage represents inflammation and symptoms originating from an irritated posterior tibial tendon, which is still functional. Stage two is characterized by a change in the alignment of the foot noted on observation while standing (see above photos). The deformity is supple meaning the foot is freely movable and a ?normal? position can be restored by the examiner. Stage two is also associated with the inability to perform a single-leg heel rise. The third stage is dysfunction of the posterior tibial tendon is a flatfoot deformity that becomes stiff because of arthritis. Prolonged deformity causes irritation to the involved joints resulting in arthritis. The fourth phase is a flatfoot deformity either supple (stage two) or stiff (stage 3) with involvement of the ankle joint. This occurs when the deltoid ligament, the major supporting structure on the inside of the ankle, fails to provide support. The ankle becomes unstable and will demonstrate a tilted appearance on X-ray. Failure of the deltoid ligament results from an inward displacement of the weight bearing forces. When prolonged, this change can lead to ankle arthritis. The vast majority of patients with acquired adult flatfoot deformity are stage 2 by the time they seek treatment from a physician.
Diagnosis
Observation by a skilled foot clinician and a hands-on evaluation of the foot and ankle is the most accurate diagnostic technique. Your Dallas foot doctor may have you do a walking examination (the most reliable way to check for the deformity). During walking, the affected foot appears more pronated and deformed. Your podiatrist may do muscle testing to look for strength deficiencies. During a single foot raise test, the foot doctor will ask you to rise up on the tip of your toes while keeping your unaffected foot off the ground. If your posterior tendon has been attenuated or ruptured, you will be unable to lift your heel off the floor. In less severe cases, it is possible to rise onto your toes, but your heel will not invert normally. X-rays are not always helpful as a diagnostic tool for Adult Flatfoot because both feet will generally demonstrate a deformity. MRI (magnetic resonance imaging) may show tendon injury and inflammation, but can?t always be relied on for a complete diagnosis. In most cases, a MRI is not necessary to diagnose a posterior tibial tendon injury. An ultrasound may also be used to confirm the deformity, but is usually not required for an initial diagnosis.
Non surgical Treatment
Get treated early. There is no recommended home treatment. While in stage one of the deformity, rest, a cast, and anti-inflammatory therapy can help you find relief. This treatment is followed by creating custom-molded foot orthoses and orthopedic footwear. These customized items are critical in maintaining the stability of the foot and ankle. Once the tendon has stretched and deformity is visible, the chances of success for non-surgical treatment are significantly lower. In a small percentage of patients, total immobilization may arrest the progression of the deformity. A long-term brace known as an ankle foot orthosis is required to keep the deformity from progressing. The Richie Brace, a type of ankle foot orthosis, shows significant success as a treatment for stage two posterior tibial dysfunction. It is a sport-style brace connected to a custom corrected foot orthodic that fits into most lace-up footwear (including athletic shoes). It is also light weight and more cosmetically appealing than traditionally prescribed ankle foot orthosis. The Arizona Brace, California Brace or Gauntlet Brace may also be recommended depending on your needs. 
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.
Adult Aquired FlatFeet Causes And Treatments
Overview
Another common term for this condition is Posterior Tibial Tendon Dysfunction (PTTD). There is a cause-effect relationship between pronation, flatfoot deformity and subsequent tenosynovitis of the posterior tibial tendon. Mechanical irritation of the tendon may lead to synovitis, partial tearing and eventually full rupture of the tendon. Other structures, including ligaments and the plantar fascia, have also been shown to contribute to the arch collapsing. As the deformity progresses, these structures have been shown to attenuate and rupture as well. In later stages, subluxation of various joints lead to a valgus rearfoot and transverse plane deformity of the forefoot. These deformities can become fixed and irreducible as significant osteoarthritis sets in.
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot. Sometimes this can be a result of specific trauma, but usually the tendon becomes injured from wear and tear over time. This is more prevalent in individuals with an inherited flat foot but excessive weight, age, and level of activity are also contributing factors.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
In diagnosing flatfoot, the foot & Ankle surgeon examines the foot and observes how it looks when you stand and sit. Weight bearing x-rays are used to determine the severity of the disorder. Advanced imaging, such as magnetic resonance imaging (MRI) and computed tomography (CAT or CT) scans may be used to assess different ligaments, tendons and joint/cartilage damage. The foot & Ankle Institute has three extremity MRI?s on site at our Des Plaines, Highland Park, and Lincoln Park locations. These extremity MRI?s only take about 30 minutes for the study and only requires the patient put their foot into a painless machine avoiding the uncomfortable Claustrophobia that some MRI devices create.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery.

Surgical Treatment
For those patients with PTTD that have severe deformity or have not improved with conservative treatments, surgery may be necessary to return them to daily activity. Surgery for PTTD may include repair of the diseased tendon and possible tendon transfer to a nearby healthy tendon, surgery on the surrounding bones or joints to prevent biomechanical abnormalities that may be a contributing factor or both.
Another common term for this condition is Posterior Tibial Tendon Dysfunction (PTTD). There is a cause-effect relationship between pronation, flatfoot deformity and subsequent tenosynovitis of the posterior tibial tendon. Mechanical irritation of the tendon may lead to synovitis, partial tearing and eventually full rupture of the tendon. Other structures, including ligaments and the plantar fascia, have also been shown to contribute to the arch collapsing. As the deformity progresses, these structures have been shown to attenuate and rupture as well. In later stages, subluxation of various joints lead to a valgus rearfoot and transverse plane deformity of the forefoot. These deformities can become fixed and irreducible as significant osteoarthritis sets in.
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot. Sometimes this can be a result of specific trauma, but usually the tendon becomes injured from wear and tear over time. This is more prevalent in individuals with an inherited flat foot but excessive weight, age, and level of activity are also contributing factors.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
In diagnosing flatfoot, the foot & Ankle surgeon examines the foot and observes how it looks when you stand and sit. Weight bearing x-rays are used to determine the severity of the disorder. Advanced imaging, such as magnetic resonance imaging (MRI) and computed tomography (CAT or CT) scans may be used to assess different ligaments, tendons and joint/cartilage damage. The foot & Ankle Institute has three extremity MRI?s on site at our Des Plaines, Highland Park, and Lincoln Park locations. These extremity MRI?s only take about 30 minutes for the study and only requires the patient put their foot into a painless machine avoiding the uncomfortable Claustrophobia that some MRI devices create.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery.
Surgical Treatment
For those patients with PTTD that have severe deformity or have not improved with conservative treatments, surgery may be necessary to return them to daily activity. Surgery for PTTD may include repair of the diseased tendon and possible tendon transfer to a nearby healthy tendon, surgery on the surrounding bones or joints to prevent biomechanical abnormalities that may be a contributing factor or both.
What May Cause Achilles Tendonitis ?
Overview
 Typically an overuse injury, Achilles tendinitis affects the connective tissue between the calf and the heel. When you walk, run or otherwise use your leg to push your body upward, the Achilles tendon is engaged. Using the tendon frequently and with high intensity often results in tendinitis -- a swollen Achilles tendon that makes it difficult and sometimes painful to continue high-impact activities.
Typically an overuse injury, Achilles tendinitis affects the connective tissue between the calf and the heel. When you walk, run or otherwise use your leg to push your body upward, the Achilles tendon is engaged. Using the tendon frequently and with high intensity often results in tendinitis -- a swollen Achilles tendon that makes it difficult and sometimes painful to continue high-impact activities.
Causes
Sometimes Achilles Tendinitis is a result of sudden trauma, as you might encounter from playing sports, but you can also have Achilles tendon pain as a result of small, unnoticed, day-to-day irritations that inflame the tendon over time by a cumulative effect. In those with no history of trauma, Achilles Tendonitis is sometimes associated simply with long periods of standing. There are several factors that can cause the gradual development of Achilles Tendinitis. Improper shoe selection, particularly using high heels over many years, increases your odds of developing the condition. This is because high-heeled shoes cause your calf muscles to contract, leaving the tendon with a lot less slack in it. Inadequate stretching before engaging in athletic or other physically-demanding activities also predisposes you to develop the problem. This is especially true in "weekend athletes", individuals who tend to partake in excessive physical activities on an intermittent basis. Biomechanical abnormalities like excessive pronation (too much flattening of the arch) also tends to cause this condition. And it is much more common individuals with equinus. It is more common in the middle-aged, the out-of-shape, smokers, and in those who use steroids. Men get the condition more frequently than women. Those involved in jumping and high-impact sports are particularly vulnerable.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
Physicians usually pinch your Achilles tendon with their fingers to test for swelling and pain. If the tendon itself is inflamed, your physician may be able to feel warmth and swelling around the tissue, or, in chronic cases, lumps of scar tissue. You will probably be asked to walk around the exam room so your physician can examine your stride. To check for complete rupture of the tendon, your physician may perform the Thompson test. Your physician squeezes your calf; if your Achilles is not torn, the foot will point downward. If your Achilles is torn, the foot will remain in the same position. Should your physician require a closer look, these imaging tests may be performed. X-rays taken from different angles may be used to rule out other problems, such as ankle fractures. MRI (magnetic resonance imaging) uses magnetic waves to create pictures of your ankle that let physicians more clearly look at the tendons surrounding your ankle joint.
Nonsurgical Treatment
Proper footwear with a strong and secure counter (the heel circumference) may help to encourage heeling of the tendon. A tendinitis will occasionally resolve on it?s own, with rest, ice, and gentle stretching. If symptoms persist for more than 2 weeks, consult your physician. Your physician may suggest physiotherapy and custom orthotics. Physiotherapy can suggest appropriate exercises and modalities to aid in the healing process. Custom orthotics can be very successful in treating the problem, as the original cause may be due to an improper alignment of the foot and heel. Re-aligning the foot to a neutral position may provide an optimal, biomechanically sound environment for healing to occur.

Surgical Treatment
If non-surgical treatment fails to cure the condition then surgery can be considered. This is more likely to be the case if the pain has been present for six months or more. The nature of the surgery depends if you have insertional, or non-insertional disease. In non-insertional tendonosis the damaged tendon is thinned and cleaned. The damage is then repaired. If there is extensive damage one of the tendons which moves your big toe (the flexor hallucis longus) may be used to reinforce the damaged Achilles tendon. In insertional tendonosis there is often rubbing of the tendon by a prominent part of the heel bone. This bone is removed. In removing the bone the attachment of the tendon to the bone may be weakened. In these cases the attachment of the tendon to the bone may need to be reinforced with sutures and bone anchors.
Prevention
Stretching of the gastrocnemius (keep knee straight) and soleus (keep knee bent) muscles. Hold each stretch for 30 seconds, relax slowly. Repeat stretches 2 - 3 times per day. Remember to stretch well before running strengthening of foot and calf muscles (eg, heel raises) correct shoes, specifically motion-control shoes and orthotics to correct overpronation. Gradual progression of training programme. Avoid excessive hill training. Incorporate rest into training programme.
Typically an overuse injury, Achilles tendinitis affects the connective tissue between the calf and the heel. When you walk, run or otherwise use your leg to push your body upward, the Achilles tendon is engaged. Using the tendon frequently and with high intensity often results in tendinitis -- a swollen Achilles tendon that makes it difficult and sometimes painful to continue high-impact activities.
Causes
Sometimes Achilles Tendinitis is a result of sudden trauma, as you might encounter from playing sports, but you can also have Achilles tendon pain as a result of small, unnoticed, day-to-day irritations that inflame the tendon over time by a cumulative effect. In those with no history of trauma, Achilles Tendonitis is sometimes associated simply with long periods of standing. There are several factors that can cause the gradual development of Achilles Tendinitis. Improper shoe selection, particularly using high heels over many years, increases your odds of developing the condition. This is because high-heeled shoes cause your calf muscles to contract, leaving the tendon with a lot less slack in it. Inadequate stretching before engaging in athletic or other physically-demanding activities also predisposes you to develop the problem. This is especially true in "weekend athletes", individuals who tend to partake in excessive physical activities on an intermittent basis. Biomechanical abnormalities like excessive pronation (too much flattening of the arch) also tends to cause this condition. And it is much more common individuals with equinus. It is more common in the middle-aged, the out-of-shape, smokers, and in those who use steroids. Men get the condition more frequently than women. Those involved in jumping and high-impact sports are particularly vulnerable.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
Physicians usually pinch your Achilles tendon with their fingers to test for swelling and pain. If the tendon itself is inflamed, your physician may be able to feel warmth and swelling around the tissue, or, in chronic cases, lumps of scar tissue. You will probably be asked to walk around the exam room so your physician can examine your stride. To check for complete rupture of the tendon, your physician may perform the Thompson test. Your physician squeezes your calf; if your Achilles is not torn, the foot will point downward. If your Achilles is torn, the foot will remain in the same position. Should your physician require a closer look, these imaging tests may be performed. X-rays taken from different angles may be used to rule out other problems, such as ankle fractures. MRI (magnetic resonance imaging) uses magnetic waves to create pictures of your ankle that let physicians more clearly look at the tendons surrounding your ankle joint.
Nonsurgical Treatment
Proper footwear with a strong and secure counter (the heel circumference) may help to encourage heeling of the tendon. A tendinitis will occasionally resolve on it?s own, with rest, ice, and gentle stretching. If symptoms persist for more than 2 weeks, consult your physician. Your physician may suggest physiotherapy and custom orthotics. Physiotherapy can suggest appropriate exercises and modalities to aid in the healing process. Custom orthotics can be very successful in treating the problem, as the original cause may be due to an improper alignment of the foot and heel. Re-aligning the foot to a neutral position may provide an optimal, biomechanically sound environment for healing to occur.
Surgical Treatment
If non-surgical treatment fails to cure the condition then surgery can be considered. This is more likely to be the case if the pain has been present for six months or more. The nature of the surgery depends if you have insertional, or non-insertional disease. In non-insertional tendonosis the damaged tendon is thinned and cleaned. The damage is then repaired. If there is extensive damage one of the tendons which moves your big toe (the flexor hallucis longus) may be used to reinforce the damaged Achilles tendon. In insertional tendonosis there is often rubbing of the tendon by a prominent part of the heel bone. This bone is removed. In removing the bone the attachment of the tendon to the bone may be weakened. In these cases the attachment of the tendon to the bone may need to be reinforced with sutures and bone anchors.
Prevention
Stretching of the gastrocnemius (keep knee straight) and soleus (keep knee bent) muscles. Hold each stretch for 30 seconds, relax slowly. Repeat stretches 2 - 3 times per day. Remember to stretch well before running strengthening of foot and calf muscles (eg, heel raises) correct shoes, specifically motion-control shoes and orthotics to correct overpronation. Gradual progression of training programme. Avoid excessive hill training. Incorporate rest into training programme.
What Is Plantar Fasciitis

Overview
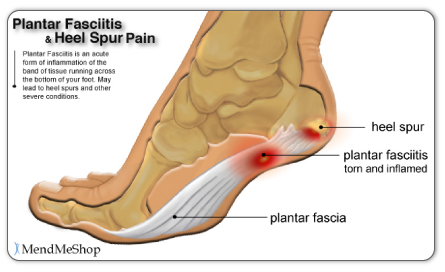
The plantar fascia is a thickened fibrous aponeurosis that originates from the medial tubercle of the calcaneus and runs forward to form the longitudinal foot arch. The function of the plantar fascia is to provide static support of the longitudinal arch and dynamic shock absorption. Individuals with pes planus (low arches or flat feet) or pes cavus (high arches) are at increased risk for developing plantar fasciitis.
Causes
Although plantar fasciitis may result from a variety of factors, such as repeat hill workouts and/or tight calves, many sports specialists claim the most common cause for plantar fasciitis is fallen arches. The theory is that excessive lowering of the arch in flat-footed runners increases tension in the plantar fascia and overloads the attachment of the plantar fascia on the heel bone (i.e., the calcaneus). Over time, the repeated pulling of the plantar fascia associated with excessive arch lowering is thought to lead to chronic pain and inflammation at the plantar fascia’s attachment to the heel. In fact, the increased tension on the heel was believed to be so great that it was thought to eventually result in the formation of a heel spur.
Symptoms
When plantar fasciitis occurs, the pain is typically sharp and usually unilateral (70% of cases).Heel pain worsens by bearing weight on the heel after long periods of rest. Individuals with plantar fasciitis often report their symptoms are most intense during their first steps after getting out of bed or after prolonged periods of sitting. Improvement of symptoms is usually seen with continued walking. Numbness, tingling, swelling, or radiating pain are rare but reported symptoms. If the plantar fascia continues to be overused in the setting of plantar fasciitis, the plantar fascia can rupture. Typical signs and symptoms of plantar fascia rupture include a clicking or snapping sound, significant local swelling, and acute pain in the sole of the foot.
Diagnosis
A physical exam performed in the office along with the diagnostic studies as an x-ray. An MRI may also be required to rule out a stress fracture, or a tear of the plantar fascia. These are conditions that do not normally respond to common plantar fasciitis treatment.
Non Surgical Treatment
Treatment of heel pain caused by plantar fasciitis begins with simple steps. There are a number of options for treatment of plantar fasciitis, and almost always some focused effort with nonsurgical treatments can provide excellent relief. In rare circumstances, simple steps are not adequate at providing relief, and more invasive treatments may be recommended. Typically, patients progress from simple steps, and gradually more invasive treatments, and only rarely is surgery required.

Surgical Treatment
If you consider surgery, your original diagnosis should be confirmed by the surgeon first. In addition, supporting diagnostic evidence (such as nerve-conduction studies) should be gathered to rule out nerve entrapment, particularly of the first branch of the lateral plantar nerve and the medial plantar nerve. Blood tests should consist of an erythrocyte sedimentation rate (ESR), rheumatoid factor, human leukocyte antigen B27 (HLA-B27), and uric acid. It’s important to understand that surgical treatment of bone spurs rarely improves plantar fasciitis pain. And surgery for plantar fasciitis can cause secondary complications-a troubling condition known as lateral column syndrome.
Stretching Exercises
Stretching exercises for the Achilles tendon and plantar fascia are recommend to relieve pain and aid in the healing process. Sometimes application of athletic tape is recommended. In moderate or severe cases of plantar fasciitis, your doctor may recommend you wearing a night splint, which will stretch the arch of your foot and calf while you sleep. This helps to lengthen the Achilles tendon and plantar fascia for symptom relief. Depending on the severity of your plantar fasciitis, your physician may prescribe a store-bought orthotic (arch support) or custom-fitted orthotic to help distribute your foot pressure more evenly.
What Leads To Plantar Fasciitis
Overview
Plantar fasciitis often occurs in middle-age. It also occurs in people who spend long hours standing on their feet at work, like athletes or soldiers. It can happen in one foot or both feet. It is common in sports like long distance running, dancing etc. Athletes who overpronate (rolling in or flattening feet) are especially at risk as the biomechanics of their feet place more stress to the band. Plantar fasciitis can take a long time to heal. Six months is the average time reported in medical research. There are some who will get cured after a few weeks and for others it will take more than a year. It can also become a chronic condition in which case some sort of treatment will always be needed to prevent the pain from coming back. As sooner as the condition is treated chances are it will not get chronic or in other words if you treat plantar fasciitis sooner you will get cured faster.
Causes
Plantar fasciitis is common in sports which involve running, dancing or jumping. Runners who overpronate where their feet roll in or flatten too much are particularly at risk the plantar fascia is over stretched as the foot flattens. A common factor is tight calf muscles which lead to a prolonged or high velocity pronation or rolling in of the foot. This in turn produces repetitive over-stretching of the plantar fascia leading to possible inflammation and thickening of the tendon. As the fascia thickens it looses flexibility and strength. Other causes include either a low arch called pes planus or a very high arched foot known as pes cavus. Assessing the foot for plantar fasciitisExcessive walking in footwear which does not provide adequate arch support has been attributed. Footwear for plantar fasciitis should be flat, lace-up and with good arch support and cushioning. Overweight individuals are more at risk of developing plantar fasciitis due to the excess weight impacting on the foot.
Symptoms
Pain is the main symptom. This can be anywhere on the underside of your heel. However, commonly, one spot is found as the main source of pain. This is often about 4 cm forward from your heel, and may be tender to touch. The pain is often worst when you take your first steps on getting up in the morning, or after long periods of rest where no weight is placed on your foot. Gentle exercise may ease things a little as the day goes by, but a long walk or being on your feet for a long time often makes the pain worse. Resting your foot usually eases the pain. Sudden stretching of the sole of your foot may make the pain worse, for example, walking up stairs or on tiptoes. You may limp because of pain. Some people have plantar fasciitis in both feet at the same time.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose plantar fasciitis. Occasionally, further investigations such as an X-ray, ultrasound or MRI may be required to assist with diagnosis and assess the severity of the condition.
Non Surgical Treatment
To alleviate the stress and pain on the fascia, the person can take shorter steps and avoid walking barefoot. Activities that involve foot impact, such as jogging, should be avoided. The most effective treatments include the use of in-shoe heel and arch cushioning with calf-stretching exercises and night splints that stretch the calf and plantar fascia while the patient sleeps. Prefabricated or custom-made foot orthotics may also alleviate fascial tension and symptoms. Other treatments may include activity modifications, NSAIDs, weight loss in obese patients, cold and ice massage therapy, and occasional corticosteroid injections. However, because corticosteroid injections can predispose to plantar fasciosis, many clinicians limit these injections. For recalcitrant cases, physical therapy, oral corticosteroids, and cast immobilization should be used before surgical intervention is considered. A newer form of treatment for recalcitrant types of plantar fasciosis is extracorporeal pulse activation therapy (EPAT), in which low-frequency pulse waves are delivered locally using a handheld applicator. The pulsed pressure wave is a safe, noninvasive technique that stimulates metabolism and enhances blood circulation, which helps regenerate damaged tissue and accelerate healing. EPAT is being used at major medical centers.

Surgical Treatment
In very rare cases plantar fascia surgery is suggested, as a last resort. In this case the surgeon makes an incision into the ligament, partially cutting the plantar fascia to release it. If a heel spur is present, the surgeon will remove it. Plantar Fasciitis surgery should always be considered the last resort when all the conventional treatment methods have failed to succeed. Endoscopic plantar fasciotomy (EPF) is a form of surgery whereby two incisions are made around the heel and the ligament is being detached from the heel bone allowing the new ligament to develop in the same place. In some cases the surgeon may decide to remove the heel spur itself, if present. Just like any type of surgery, Plantar Fascia surgery comes with certain risks and side effects. For example, the arch of the foot may drop and become weak. Wearing an arch support after surgery is therefore recommended. Heel spur surgeries may also do some damage to veins and arteries of your foot that allow blood supply in the area. This will increase the time of recovery.
Prevention
Every time your foot strikes the ground, the plantar fascia is stretched. You can reduce the strain and stress on the plantar fascia by following these simple instructions: Avoid running on hard or uneven ground, lose any excess weight, and wear shoes and orthotics that support your arch to prevent over-stretching of the plantar fascia.
What Leads To Heel Pain To Flare Up

Overview
Plantar fasciitis causes pain in the bottom of the heel. The plantar fascia is a thin ligament that connects your heel to the front of your foot. It supports the arch in your foot and is important in helping you walk. Plantar fasciitis is one of the most common orthopedic complaints. Your plantar fascia ligaments experience a lot of wear and tear in your daily life. Normally, these ligaments act as shock absorbers, supporting the arch of the foot. Too much pressure on your feet can damage or tear the ligaments. The plantar fascia becomes inflamed, and the inflammation causes heel pain and stiffness.
Causes
Plantar fasciitis is caused by straining the ligament that supports your arch. Repeated strain can cause tiny tears in the ligament. These can lead to pain and swelling. This is more likely to happen if your feet roll inward too much when you walk, you have high arches or flat feet. You walk, stand, or run for long periods of time, especially on hard surfaces. You are overweight. You wear shoes that don't fit well or are worn out. You have tight Achilles tendons or calf muscles.
Symptoms
Most patients with plantar fasciitis describe a sharp or stabbing pain on the bottom of the heel that is most severe when they first get up in the morning or after a period of resting. Some may feel like the heel is bruised while others may describe tightness or even a pulling sensation on the heel or arch.
Diagnosis
To diagnose plantar fasciitis, your doctor will physically examine your foot by testing your reflexes, balance, coordination, muscle strength, and muscle tone. Your doctor may also advise a magnetic resonance imaging (MRI) or X-ray to rule out other others sources of your pain, such as a pinched nerve, stress fracture, or bone spur.
Non Surgical Treatment
Treatment initially involves offloading the plantar fascia by aoiding aggravating factors, such as running. Taping, this can work very well to alleviate pain, and can be almost immediate. It isn't a long-term solution, but can relieve symptoms in the beginning. Using a night splint to stretch the calf, so that less load is placed on the plantar fascia (if tightness in the calf is a factor). Using a gel heel cup, this can act to increase shock absorption, and by raising the heel there is also less stretch on the calf. So, temporarily, this may relieve pain in someone who has a tight calf. Massage, but this depends if the plantarfascia is actually tight or just painful. If it is tight, then massage can temporarily relieve the pain, but if it is irritated then taping and corrective footwear is preferable.

Surgical Treatment
If you consider surgery, your original diagnosis should be confirmed by the surgeon first. In addition, supporting diagnostic evidence (such as nerve-conduction studies) should be gathered to rule out nerve entrapment, particularly of the first branch of the lateral plantar nerve and the medial plantar nerve. Blood tests should consist of an erythrocyte sedimentation rate (ESR), rheumatoid factor, human leukocyte antigen B27 (HLA-B27), and uric acid. It’s important to understand that surgical treatment of bone spurs rarely improves plantar fasciitis pain. And surgery for plantar fasciitis can cause secondary complications-a troubling condition known as lateral column syndrome.
Stretching Exercises
Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It's usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Towel stretches. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Wall stretches. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stair stretches. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Chair stretches. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. Dynamic stretches. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day.